Nick specialises in open and laparoscopic (keyhole) surgery for the resolution of hernias. With over 30 years experience, Nick has performed more than 3,000 procedures and operations using either an open, totally extraperitoneal (TEP) or transabdominal preperitoneal (TAPP) laparoscopic approach.
Hernias can occur all over the body, but most commonly affect the abdomen. Those that do are usually caused by weakness in the muscle layer of the abdominal wall. This then allows an organ to migrate through that weakness to a part of the body where it should not be present.
Approximately 75,000 people in the UK undergo surgery to repair inguinal hernias every year (95% are men).
What is an inguinal hernia?
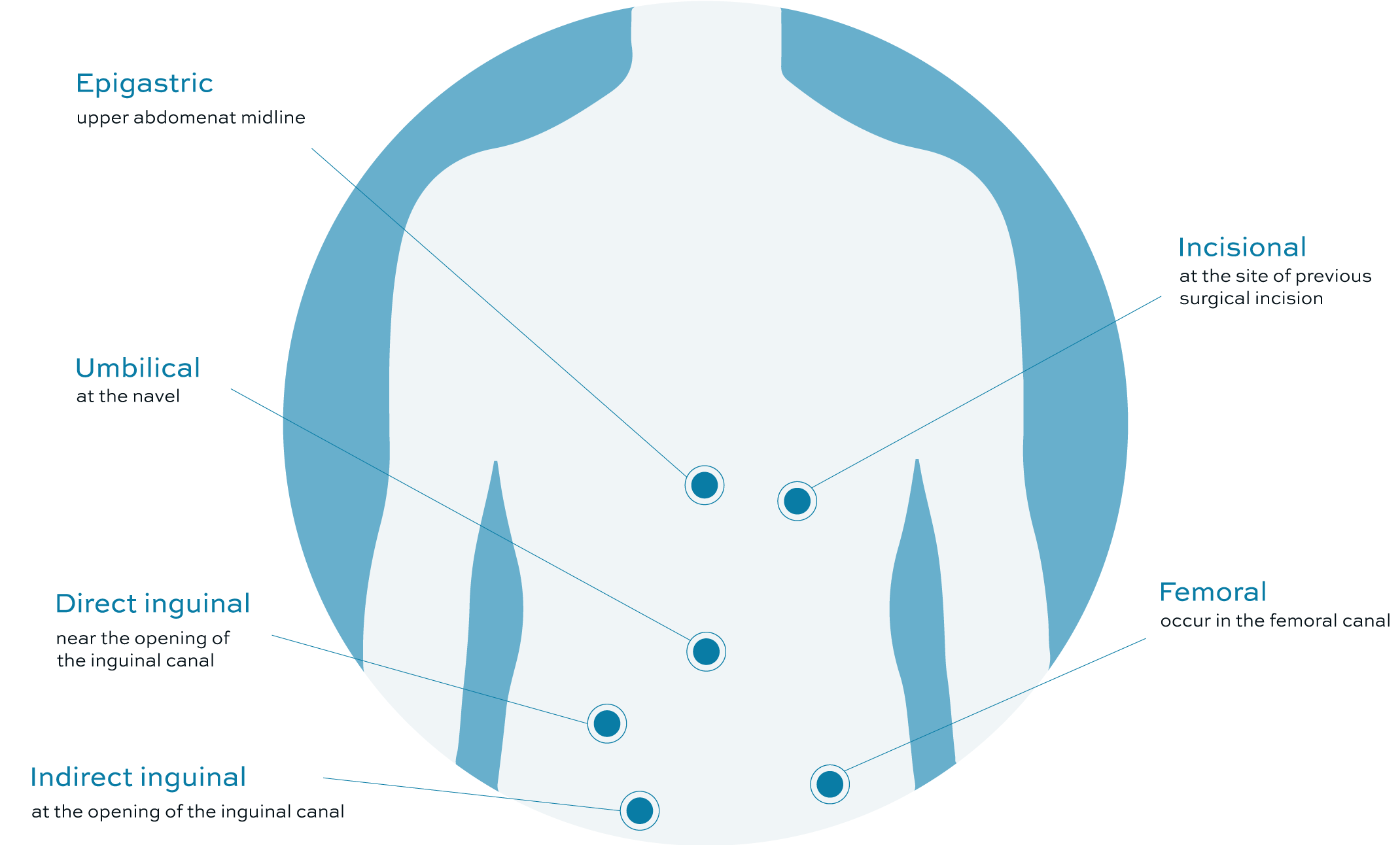
There are essentially two kinds of inguinal hernia.
Indirect inguinal hernias can occur at any age as a result of failure of closure of the “deep inguinal ring” following descent of the testicle through it on its way from the abdominal cavity into the scrotum. These hernias in particular are more likely to result in pain and strangulation.
Direct inguinal hernias occur as a consequence of degeneration and weakness in the fascia and muscular layer of the abdominal wall in the inguinal canal. Men are ten times as likely to suffer from direct inguinal hernias and usually these occur in middle and old age.
Causes
Indirect inguinal hernias result from a congenital weakness. This may present at any age and often run in families. Appearance of both direct and indirect inguinal hernias may be precipitated by the following:
- Increased pressure within the abdomen.
- Heavy lifting and straining.
- Pregnancy.
- Chronic cough.
More often than not there is no obvious precipitating factor.
Symptoms can vary, but can include the following:
Uncomplicated Inguinal Hernia – Signs and Symptoms
Intermittent lump in the groin usually more apparent upon standing up or coughing.
Pain in the groin which may or may not be associated with a lump.
Dragging sensation or a feeling of “pressure” in the groin.
Discomfort in the testicle and when hernias enlarge a lump protruding into the scrotum from the groin.
Incarcerated Inguinal Hernia – Signs and Symptoms
Usually it is possible if a lump exists to massage it back inside the abdomen without difficulty. However, occasionally structures, including parts of the bowel, can become trapped within the hernia sac. This can lead to a strangulated hernia in which the bowel loses its blood supply and is at risk of dying. This is a potentially life-threatening event requiring emergency surgery. Studies have failed to identify any specific signs and symptoms which may predict this event. The risk however is low but probably increases the longer a hernia is left untreated.
Symptoms of a strangulated hernia would include:
- Sudden and increased pain in the groin.
- The lump becomes painful and irreducible.
- The lump may become hot and red.
- Abdominal pain, nausea and vomiting.
- Fever, sweating or rapid heart rate.
In the event of any of the above occurring emergency medical advice should be sought immediately.
Sportsman’s Hernias
There remains controversy regarding chronic discomfort in the groin in which there is no definite lump. This often occurs in young, fit, sportsmen and is precipitated by physical activity. Investigations may include physical examination, ultrasound or MRI scans, all of which are designed to exclude other soft tissue injury. Your surgeon may then advise undergoing a diagnostic laparoscopy to identify a small hernia.
More often than not a history and physical examination is all that is required to diagnose an inguinal hernia.
On occasions where the diagnosis is less clear further tests may be requested including ultrasound, MRI or CT scans.
Treatment options
There are various treatment options for inguinal hernias. Here are the principal ones.
Watchful waiting
If your hernia is small and causing no symptoms one option would be to watch and wait. However the natural history of these hernias is that they all do tend to increase in size over time and there is always an unpredictable risk of strangulation. The decision to operate will be made between you and your surgeon following discussion of the risks and benefits.
Surgery
Surgery has been performed to repair groin hernias for nearly 150 years and many procedures have been described. Until about thirty years ago all operations involved suturing tissues together. This carries a high risk of both recurrence (hernias occur again at some point following this surgery) as well as high levels of chronic discomfort and pain. Consequently today the majority of surgeons employ the use of “plastic mesh”. There are many different meshes but they are all employed to repair the defect in the anterior abdominal wall. Over time scar tissue grows into this scaffolding and provides a long term strong repair.
Mesh is employed in all modern surgical techniques and should allow much more rapid recovery following your operation than in the past. Whichever of the following operative techniques is used, 80% of patients will return home on the day of their surgery.
We offer the full range of surgical techniques and following consultation you will be offered the most appropriate procedure for you, including taking into account your preferred choice. Most patients are offered totally extra-peritoneal laparoscopic repair as we believe this provides the most rapid post operative recovery as well as the best outcome for you the patient. Collected data from our patients show currently median time to resumption normal activities and work as 8 days (range 0-21).
Open Hernia Repair
This is the most widely employed technique in the United Kingdom. It requires an incision in the groin and the use of usually plastic mesh to repair the defect. This operation carries the advantages that it is simple to undertake, requires minimal technology and if necessary can be performed under local anaesthetic.
Laparoscopic Procedures
These minimally invasive procedures carry the advantage of rapid post operative recovery. Patients often experience minimal discomfort following surgery and can therefore resume normal activities rapidly. Multiple studies have compared laparoscopic and open techniques and almost all have confirmed more rapid convalescence and return to normal activities following laparoscopic procedures.
Laparoscopic operations carry the significant advantage that patients with hernias on both sides can be treated at the same time with minimal additional discomfort. Some patients present with recurrent hernias following failure of a previous operation. Laparoscopic repair is the procedure of choice in these patients as the risk of damaging nerves and blood vessels supplying the testicle are lower.
Laparoscopic surgery may not be for you if:
- Your hernia is very large.
- Your hernia is incarcerated.
- You have had previous pelvic surgery including prostatectomy.
- You are unfit for general anaesthesia.
There are two kinds of laparoscopic operation:-
Totally Extra-peritoneal (TEP)
This is an advanced laparoscopic procedure. The surgery is performed through very small incisions whilst visualisation is accomplished with the use of a telescope and high resolution camera. Following reduction of the hernia, prosthetic mesh is placed behind the defect to prevent recurrence. This procedure has the advantage that, as the abdominal cavity is not actually entered and the surgery is undertaken between the peritoneum and abdominal wall muscles, you should not experience shoulder tip pain. Also injury to other organs within the abdomen is probably lower.
Trans-abdominal Pre-peritoneal (TAPP)
This is similar to TEP but the abdominal cavity is entered before the hernia is reduced. Consequently patients can experience shoulder pain because of gas within the abdominal cavity and there is a theoretical risk to internal abdominal organs.
Recovery
Following modern hernia surgery, the recovery is quicker. However, there is strong evidence which reflects our experience that following laparoscopic operations patients recover more rapidly than after open operations. Typically following a totally extraperitoneal laparoscopic repair, on average patients will be up and moving around, returning to normal daily activities within a fortnight.